CANADA: According to a cluster-randomized trial reported in The New England Journal of Medicine, patients with refractory ventricular fibrillation (VF) were more likely to survive to hospital discharge utilizing double sequential external defibrillation (DSED) and vector-change (VC) defibrillation than those who received the conventional approach.
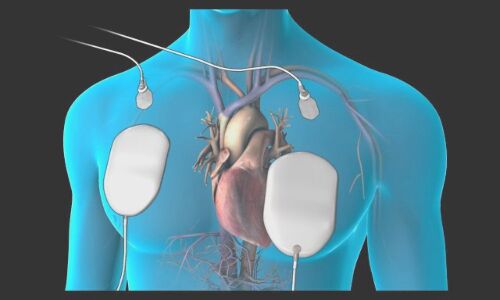
Shock-refractory ventricular fibrillation, which occurs during out-of-hospital cardiac arrest, is still widespread despite advancements in defibrillation technology. Rapidly spaced shocks from two defibrillators make up DSED. Defibrillation pads are moved from the anterior-lateral to the anterior-posterior position during VC defibrillation. To enhance outcomes for individuals with refractory ventricular fibrillation, these defibrillation techniques have been proposed.
The study’s objective was to compare conventional defibrillation to DSED and VC defibrillation in adult patients experiencing out-of-hospital cardiac arrest with refractory ventricular fibrillation.
This trial was carried out in six Canadian paramedic organizations on adults who experienced out-of-hospital cardiac arrest and refractory ventricular fibrillation.
Three typical defibrillation attempts were made on each subject. After three successive shocks, those who were still in ventricular fibrillation were given one of the three defibrillation techniques that the paramedic service was randomly allocated to use. Prior to the COVID-19 pandemic, a total of 405 patients (mean age, 63.6 years; 84% men) were enrolled in the trial. Bystanders saw 68% of out-of-hospital cardiac arrests, and 58% of those patients got bystander CPR. The three groups shared similar resuscitation characteristics and a median delay of roughly 10 minutes between the initial call and the first defibrillation.
The main result was staying alive until being released from the hospital. Secondary outcomes were the cessation of ventricular fibrillation, restoration of spontaneous circulation, and a positive neurologic outcome, defined as a modified Rankin scale score of 2 or lower (meaning no symptoms to mild disability) at hospital discharge.
Key findings of the trial:
- The DSED group had a higher rate of survival to hospital discharge than the standard group (30.4% vs. 13.3%; relative risk, 2.21; 95% confidence interval [CI], 1.33 to 3.67)
- the VC group had a higher rate of survival than the standard group (21.7% vs. 13.3%; relative risk, 1.71; 95% CI, 1.01 to 2.88).
- In comparison to standard defibrillation, DSED, but not VC defibrillation, was linked to a larger proportion of patients having a favorable neurologic outcome (relative risks, 2.21 [95% CI, 1.26 to 3.88] and 1.48 [95% CI, 0.81 to 2.71], respectively).
- Return of spontaneous circulation occurred in 46.4% against 26.5%, and ventricular fibrillation was terminated in 84% of the DSED group versus 67.6% of the conventional group (RR, 1.25). (RR, 1.72).
- In the VC group, recovery of spontaneous circulation happened in 35.4% of cases while ventricular fibrillation termination occurred in 79.9% of cases, yielding an RR of 1.18 compared to traditional defibrillation (RR, 1.39).
The investigators claimed that all patients with refractory ventricular fibrillation should certainly consider either double defibrillation or an alternative pad placement.
“To further understand the effects of DSED and VC defibrillation for refractory ventricular fibrillation, more investigation is required. This should include trials that are explicitly powered to compare the two methods and those that take post-resuscitation care into account,” they continued.
The authors concluded that until then, “such protracted types of defibrillations are not ready for routine therapy, although they may be taken into consideration when no other therapeutic alternatives remain.”
REFERENCE
Cheskes S, Verbeek PR, Drennan IR, McLeod SL, Turner L, Pinto R, Feldman M, Davis M, Vaillancourt C, Morrison LJ, Dorian P, Scales DC. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. 2022 Nov 6. doi: 10.1056/NEJMoa2207304. Epub ahead of print. PMID: 36342151.